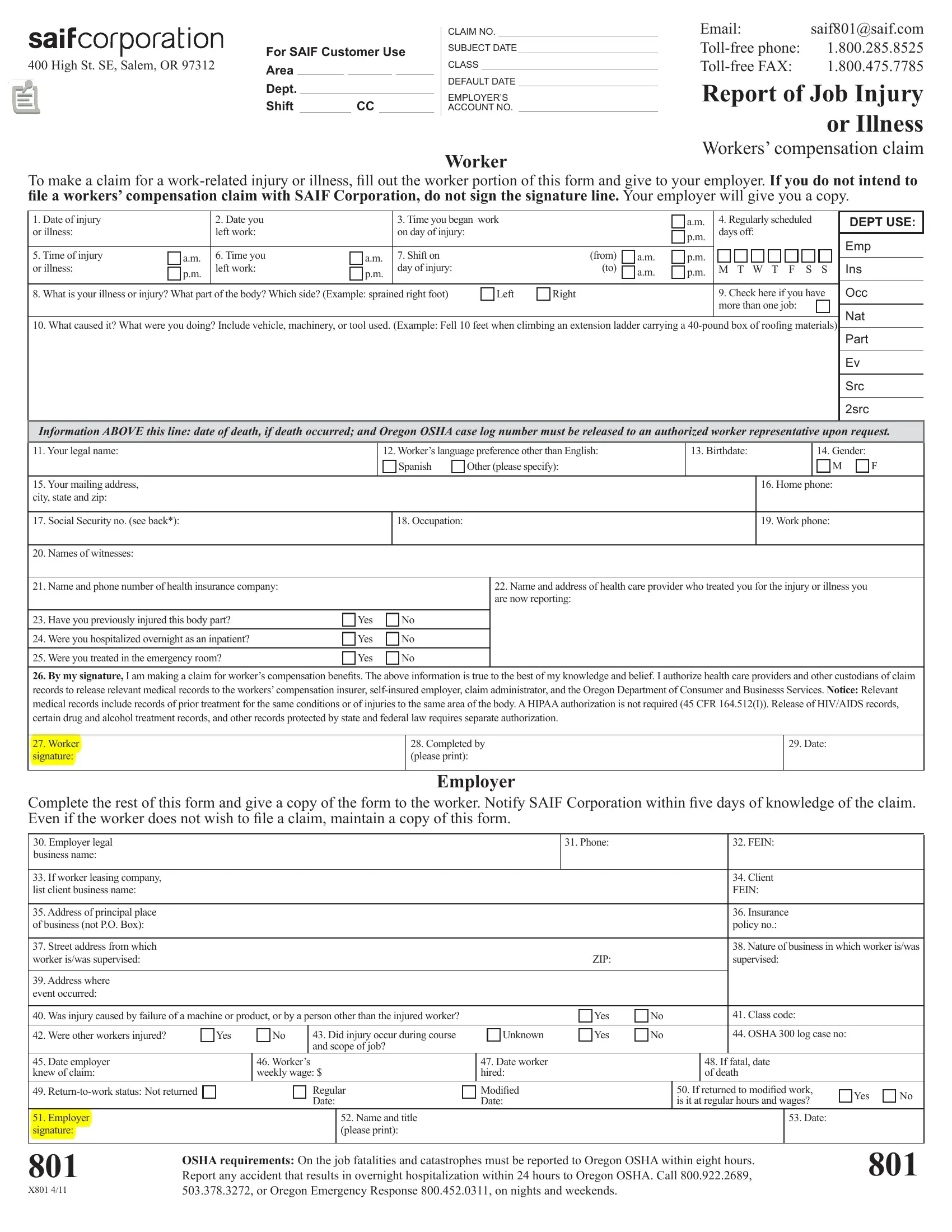
Navigating the procedural steps following a work-related injury or illness can seem daunting for employees and employers alike. The Saif 801 form, a critical document for initiating workers' compensation claims within the framework of SAIF Corporation's requirements, serves as a starting point in this journey. Designed for the prompt reporting of occupational injuries or illnesses, this form captures essential details about the incident, from the date and time of occurrence to a description of the injury and its causation. It further delves into the worker's personal information, workplace specifics, and the immediate actions taken post-incident, such as medical treatment received. Particularly noteworthy is its inclusion of directives for both the injured worker and the employer, emphasizing responsibilities like notifying SAIF Corporation within a stipulated timeframe and maintaining records even if a claim is not filed. Additionally, the form provides guidance on navigating subsequent steps, like seeking medical treatment and understanding the implications of lost wages due to work incapacity. Moreover, it underscores the importance of accurate and truthful claim filing, highlighted by the requirement for the worker's signature under the assertion that the information provided is correct to the best of their knowledge. The form also accommodates workers with language preferences other than English, reflecting an inclusive approach toward ensuring comprehensibility and accessibility in the claims process. This initial form is part of a larger ecosystem designed to streamline the interaction between workers, employers, and SAIF Corporation, ultimately aimed at facilitating efficient and equitable resolutions to workers' compensation claims.
| Question | Answer |
|---|---|
| Form Name | Saif 801 Fillable Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | saif form 801, saif 801, corters saif 31 01 be ofeso, printable 801 form |