
Dealing with PDF documents online is actually quite easy with this PDF tool. Anyone can fill in va disability form for diabetes here and use several other options available. Our team is aimed at providing you with the best possible experience with our tool by continuously presenting new functions and enhancements. With these improvements, using our editor gets easier than ever! If you are looking to get going, here is what it's going to take:
Step 1: Click on the "Get Form" button at the top of this page to open our editor.
Step 2: With this advanced PDF tool, it is easy to accomplish more than just fill out blank fields. Try each of the features and make your docs appear faultless with custom textual content added, or modify the original content to perfection - all supported by an ability to incorporate any kind of images and sign it off.
As for the fields of this particular PDF, here's what you need to know:
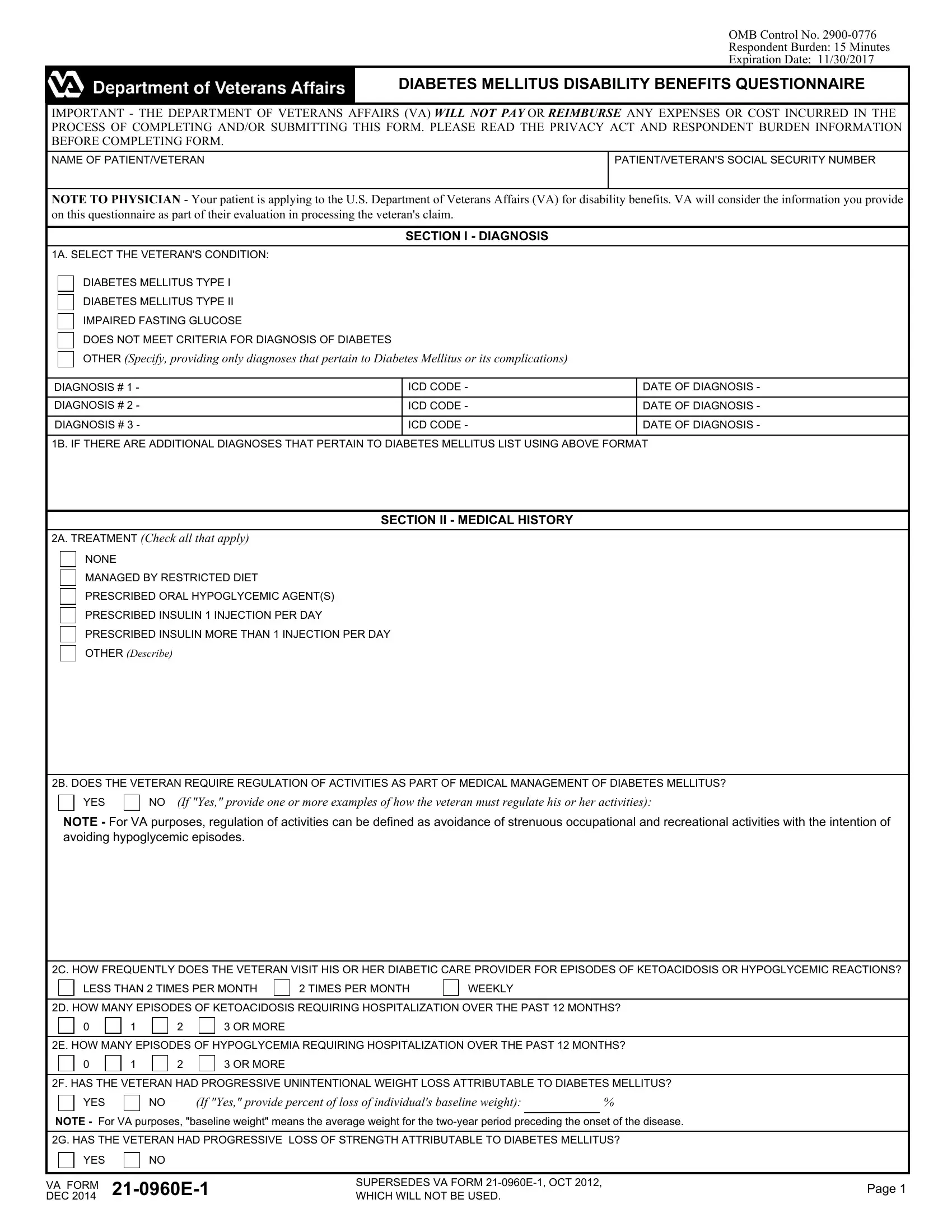
1. To start off, once filling out the va disability form for diabetes, start in the section that includes the next fields:
Step 3: Soon after going through your fields you've filled in, hit "Done" and you're all set! Join FormsPal today and easily get access to va disability form for diabetes, all set for download. All alterations you make are preserved , making it possible to customize the document further anytime. FormsPal is invested in the personal privacy of our users; we make sure that all personal data entered into our editor stays confidential.