
How to Complete the Allstate Appeal Form
Follow these steps to fill out and submit your Allstate Appeal Form correctly:
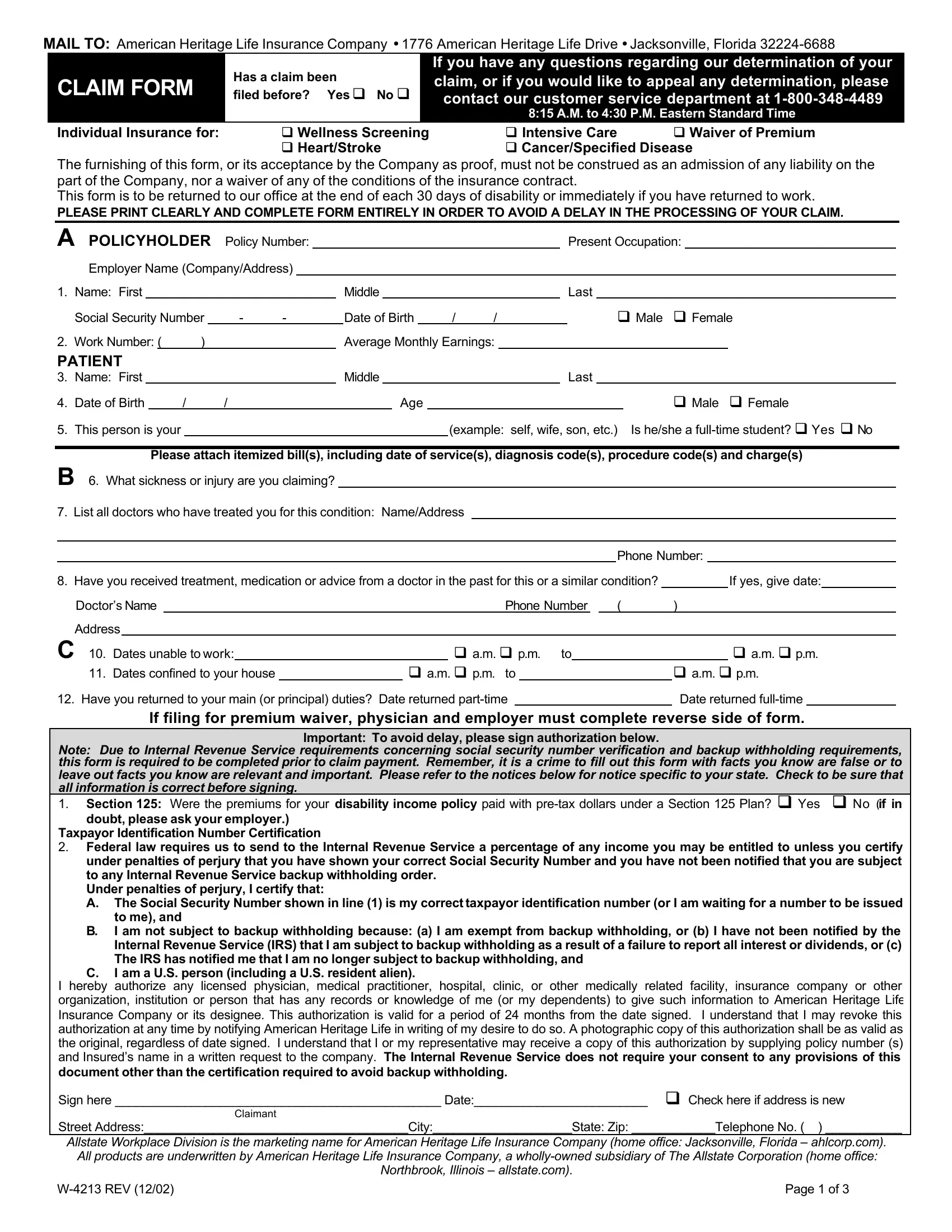
- Gather your documents. Before filling out the form, collect your insurance policy number, the original claim denial letter, and any supporting evidence such as medical records, physician statements, or receipts.
- Fill in policyholder details. Enter your full name, mailing address, date of birth, and policy number in the fields at the top of the form.
- Describe your appeal. In the explanation section, clearly state why you disagree with the claim decision. Include the date of the original decision, specific coverage types involved, and a factual account of the dispute.
- Attach supporting documentation. Include all relevant documents with your form: physician statements, diagnosis codes, itemized bills, and any prior authorizations related to your claim.
- Sign and date the form. Your signature certifies the accuracy of the information provided. If you are filing on behalf of another person, attach the required written authorization.
- Submit the completed form. Send the form and all attachments to the mailing address or fax number listed in your denial letter. Keep a copy of everything for your records.
Common Questions About the Allstate Appeal Form
What is the deadline for filing an Allstate appeal?
The deadline is typically stated in your claim denial letter. Most Allstate policies require the appeal to be submitted within 180 days of receiving the denial notice. Check your specific policy for the exact timeframe that applies to your coverage.
What types of claims can I appeal using this form?
The Allstate Appeal Form covers claims related to Wellness Screening, Intensive Care, Waiver of Premium, Heart/Stroke, and Cancer/Specified Disease insurance coverages distributed through the Allstate Workplace Division. If your claim type is not listed, contact Allstate directly to confirm which form applies.
Can I file an appeal on behalf of a family member?
Yes. If you are an authorized representative or designee, you may complete and sign the appeal form on behalf of the policyholder. Include documentation confirming your authorization with the submission.
Where do I send the completed Allstate Appeal Form?
The submission address or fax number is listed in your original claim denial letter. If you cannot locate this information, contact Allstate customer service for the correct mailing address for your specific coverage type.
For additional insurance appeal resources, review the Aetna Appeal Form if your claim involves a secondary insurer, or use the general Appeal Form template for other insurance providers. The Appeal Request Form is another option for formal appeal submissions.