Completing the CS-274W form online is straightforward using the FormsPal PDF editor. Our tool lets you open, review, and fill in the child care provider enrollment form directly in your browser without downloading extra software. Follow the four steps below to get started:
Step 1: Click the orange "Get Form Now" button at the top of this page. The CS-274W form will open in the FormsPal online PDF editor, ready for you to complete.
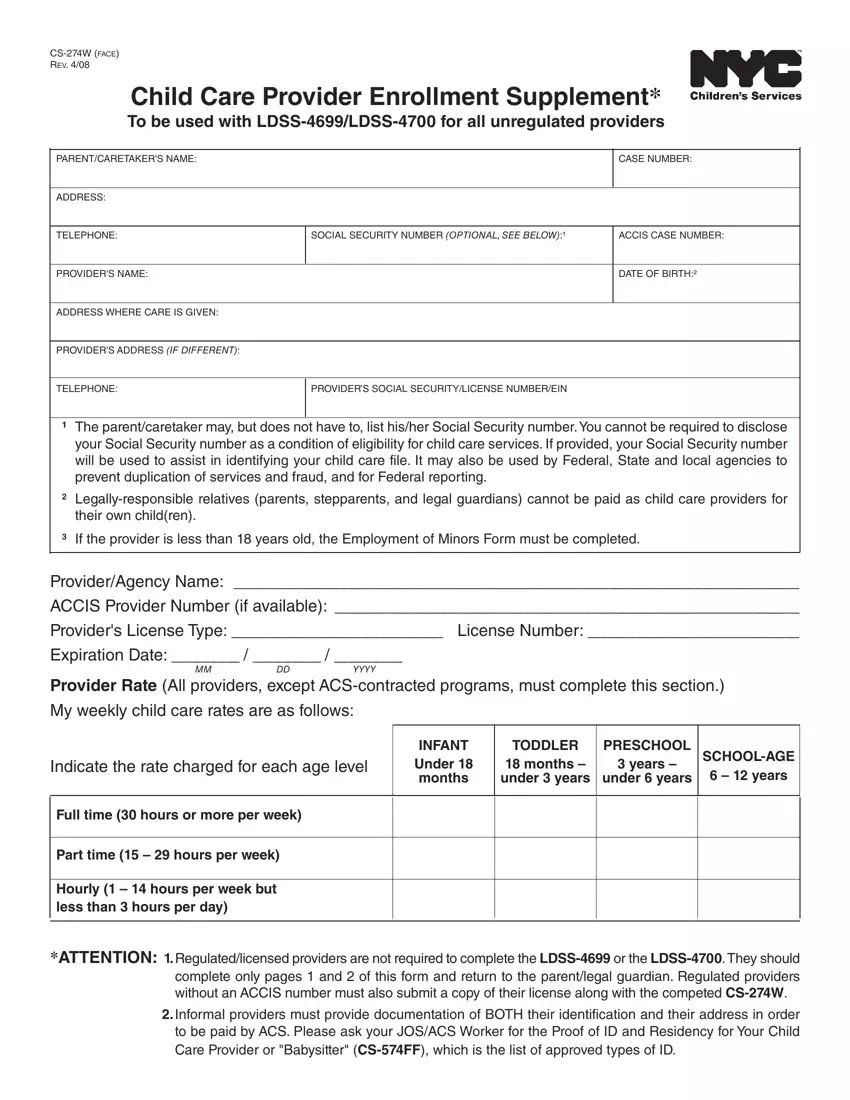
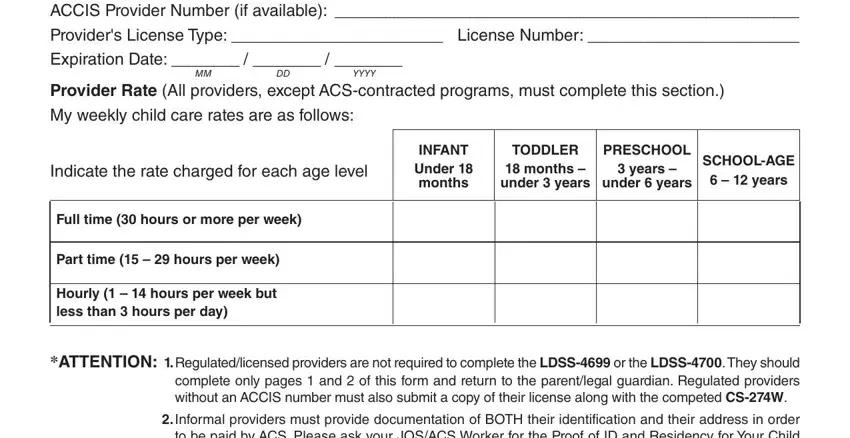
Step 2: Once the form is open, review the editing toolbar at the top of the page. You can add text, check boxes, insert dates, and use other tools to fill in each required field. Start with the provider or agency name, the program year, and the applicable child care rates for each age group and care type. Fill in the rate fields for infant, toddler, preschool, and school-age care, across full-time, part-time, and hourly service categories.
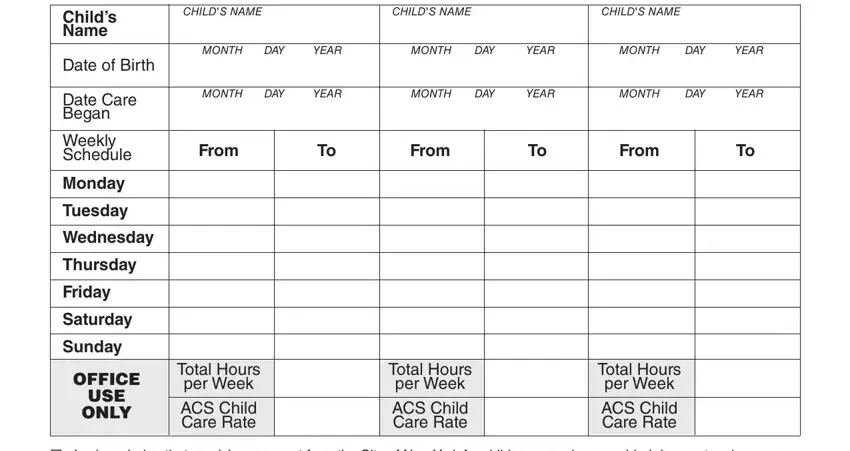
In the child care schedule section, enter the child's name, date of birth, and the date care began. Then complete the weekly schedule by listing each day and the hours the provider will care for the child. If the provider cares for more than one child under this enrollment, fill in one row per child in the schedule section.
The provider certification and parent or guardian certification sections appear at the bottom of the form. The provider signs and dates to confirm they are not a city employee or a relative of the child. The parent or guardian signs to confirm the information is accurate and the care arrangement is legitimate under the New York City child care subsidy program guidelines.
Step 3: Once you have completed all required fields and reviewed the form for accuracy, click the "Done" button to save your completed CS-274W form as a PDF file ready for submission.
Step 4: Download your completed PDF and keep a copy for your own records before submitting the original to the ACS or HRA office. FormsPal does not store or share your personal information.
Tips for Completing the CS-274W Form
Keep the following points in mind when filling out the child care provider enrollment supplement to avoid delays or errors in your subsidy application:
- Use your actual current provider rates. ACS uses the rates listed on this form to calculate the reimbursement amount, so enter the real rates you charge rather than estimated or rounded figures.
- Always submit the CS-274W alongside the LDSS-4699 or LDSS-4700 forms. The enrollment supplement is not a standalone document and must accompany the primary enrollment application to be processed.
- Keep copies of all documents you submit to ACS for your own records, including the CS-274W form, your enrollment application, and any supporting documents requested by the HRA office handling your case.
- If you provide care for children across different age groups, complete each rate row that applies to your situation. Leave blank any row for an age group you do not currently serve.
- Notify the HRA or ACS office promptly if your rates, schedule, or care arrangement changes after you submit the form. Changes to your enrollment details may require a new or updated CS-274W form.
Frequently Asked Questions About the CS-274W Form
What does CS-274W stand for?
CS-274W is the form number assigned by New York City's Human Resources Administration. The form is officially titled the Child Care Provider Enrollment Supplement and is used to enroll unregulated child care providers in the city's subsidized child care program.
Who fills out the CS-274W form?
Both the child care provider and the parent or caretaker must complete and sign the CS-274W form. The provider completes the rates and child care schedule sections, while the parent or guardian completes the certification section confirming the care arrangement is legitimate and the information is accurate.
How do I submit the completed CS-274W form?
Submit the completed CS-274W form to the New York City HRA or ACS office handling your child care subsidy case. The form is typically submitted together with the LDSS-4699 or LDSS-4700 enrollment forms and any additional documents requested by your caseworker. Contact your local HRA office to confirm the required documents for your specific case.
Can I fill out the CS-274W form online?
Yes. You can complete the CS-274W form using the FormsPal online PDF editor on this page. Click the "Get Form Now" button to open the form, fill in the required fields using the editing tools, and download your completed PDF for submission to the HRA or ACS office.
What happens if information on the CS-274W form changes?
If your child care rates, schedule, or other enrollment details change after you submit the CS-274W form, you must notify the HRA or ACS office handling your case. You may be required to complete and submit a new or updated CS-274W form to reflect the change. Failure to report changes in a timely manner may affect your reimbursement or program eligibility.
Is the CS-274W form available in other languages?
New York City's HRA provides many child care program documents in multiple languages, including Spanish and Haitian Creole, to serve the city's diverse population. Contact your local HRA office or visit the NYC HRA website to request the CS-274W form or related documents in your preferred language.
