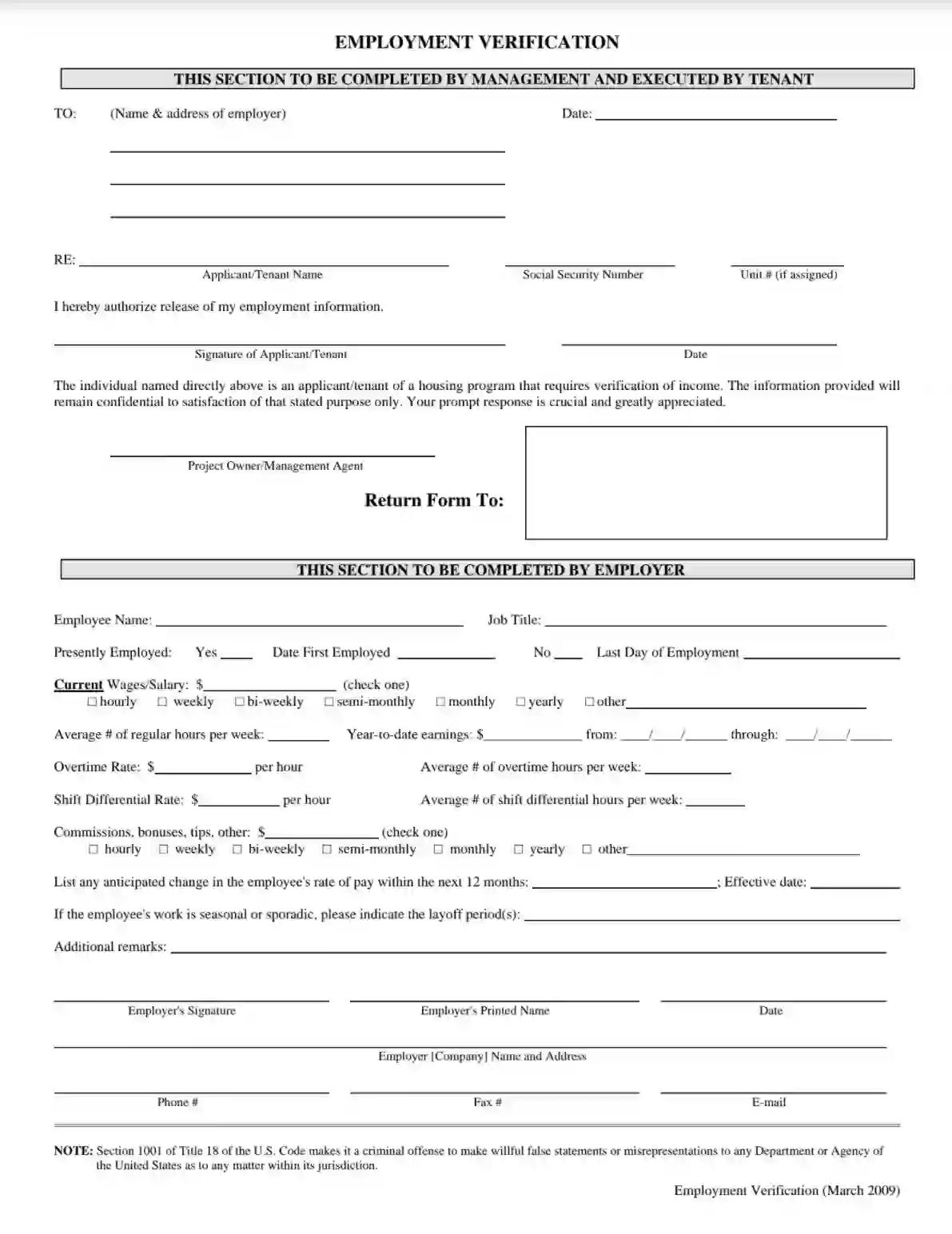
The Employment Verification Form confirms an individual’s employment status and income, typically requested by management or housing programs. The form is divided into two main sections: one for management to complete and another for the employer. The management section includes tenant authorization to release their employment information, emphasizing confidentiality and prompt response. The employer section requires detailed information about the employee, such as employment status, job title, salary, hours worked, and any additional earnings like overtime or bonuses. This form authenticates an employee’s financial stability and employment details, which is crucial for securing housing or verifying income for loan applications.
Other Employment Forms
Do you need other employment PDF forms? Check out the selection following next to see what you may fill in and edit with FormsPal. Also, remember that you can actually upload, fill out, and edit any PDF document at FormsPal.
We encourage you to generate, fill in, and download the required income verification template via our PDF file-building online tools. As employment letters are created for various reasons, like financing or housing programs, the templates may also vary. We have tailored an illustrated guide below to make it effortless for you to prepare the needed documentation.
Some forms contain distinct structures, designating the individual who is eligible to execute each part. However, if the composition is more of an agreement — no worries. Employment verification reports are relatively free forms and concede differences.
Place the Date
Begin tailoring the form by specifying the calendar date when the referenced document is prepared.
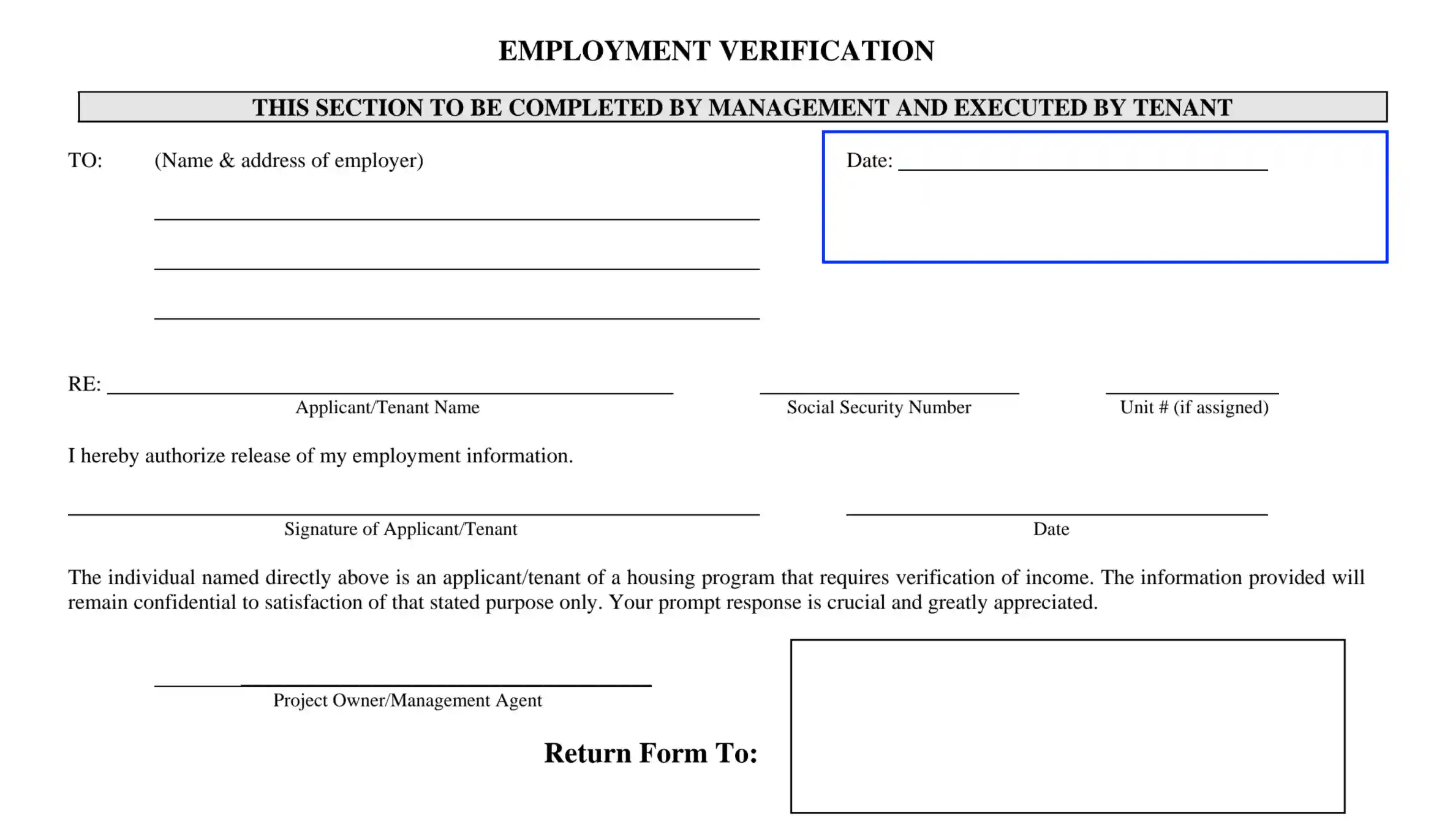
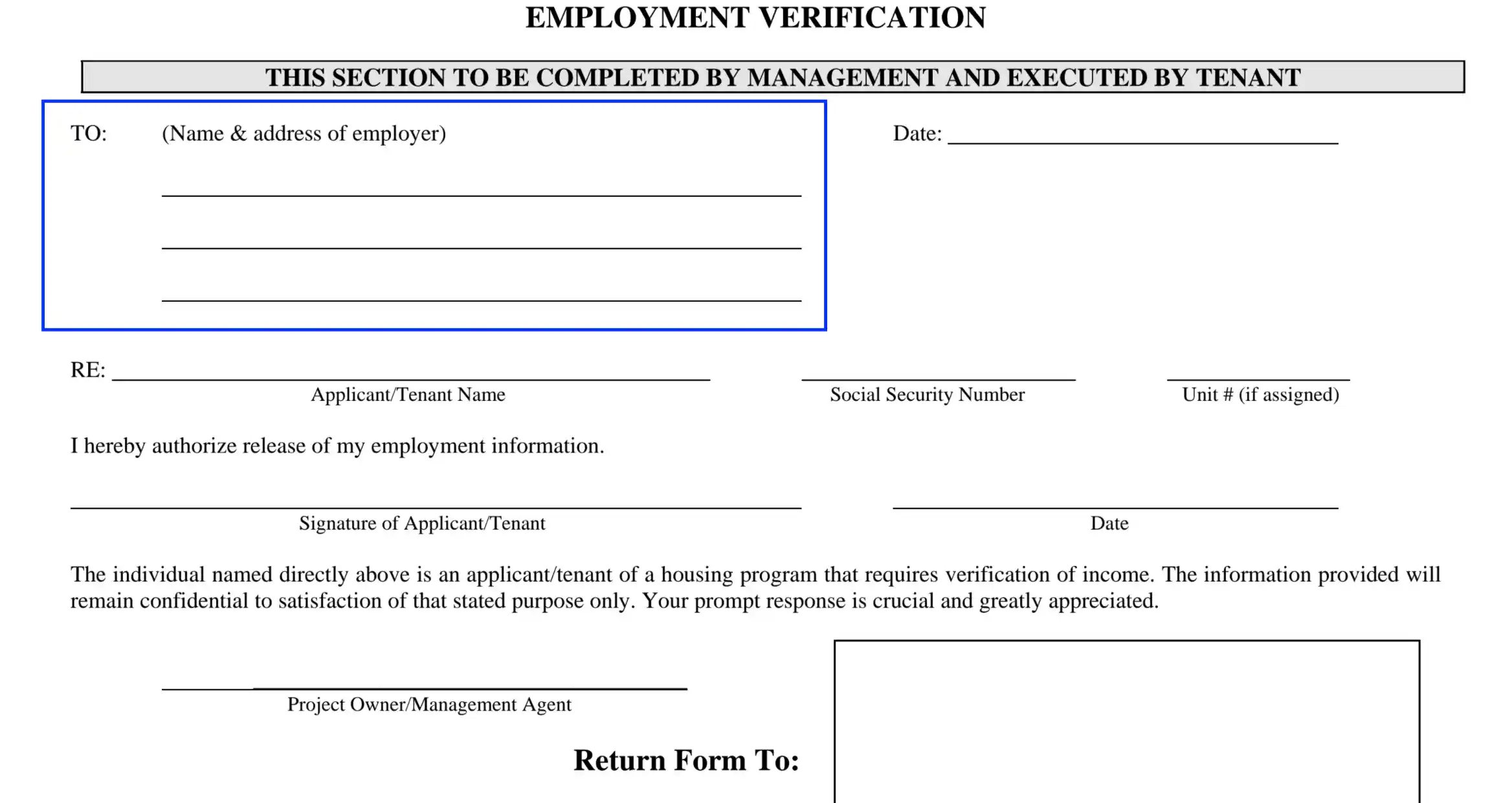
Define the Employer
Here, the preparer needs to enter the employer’s name and physical address. List the street and suite (or its alternative) number, city, state, and ZIP details.
Identify the Employee
Up next, the preparer needs to enter the employee’s (as a rule, the applicant’s) working data. List the following parameters:
Authorize the Employer
Collect the employee’s signature and place the current date to confirm their consent to disclose the confidential employment info.
Specify the Program’s Supervisor
Complete the heading part by identifying the manager who supervises the financing, housing, or another type of program. Enter the agent’s name and signature (if needed).
Define the Recipient
Submit the recipient’s details to whom the form is returned after the verification is completed. List the individual’s full name and mailing address or P. O. Box details.

Once the heading info is ready, the preparer can proceed to fill out the employee’s data. Let the employer or HR department complete the required information.
Submit the Employee’s Details
Here, the preparer should enter the employee’s legal name and position they have.
Describe the Employee’s Working Background
In this section, you are encouraged to clarify if the applicant is employed by the referenced employer currently. If “Yes,” enter the date of recruitment. In case the applicant appears to be a former employee, enter the date they performed the duties last.
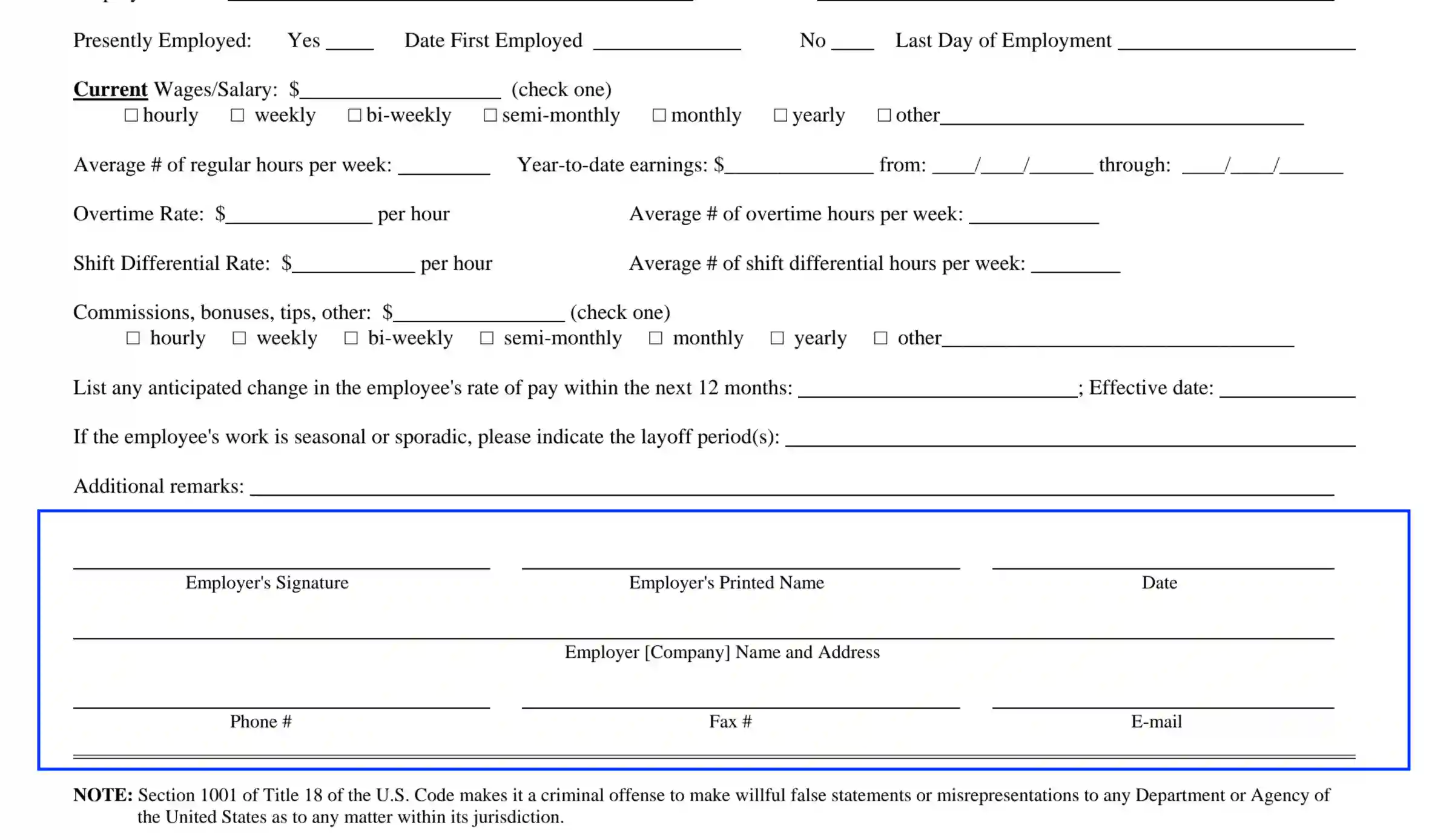
Submit the Applicant’s Income
Dedicate this section to cover earnings-related aspects. List the income amounts in US dollars as follows:
Define Changes in the Rate of Payment (If Applicable)
If the employer plans to amend the applicant’s payment rate within the upcoming year, enter the anticipated adjustments in this unit. Also, specify the calendar date when the changes come into force.
Specify the Applicant’s Working Schedule
Here, the employer needs to clarify whether the applicant is employed by periods. In case the employee fulfills their duties seasonally, enter the schedule details or periods.

Enter Extra Data (If Applicable)
If there is any inherent information related to the applicant’s duties, responsibilities, and reimbursements the employer would like to share with the program supervisors, use this section to give a short description.
Collect the Employer’s Signature and Business Data
The final step lies in appending the employer’s signature and the entity’s (proprietor’s) business details. Confirm the disclosed info by providing the required data as follows: