
Should you desire to fill out the Ambetter Inpatient Prior Authorization form online, it is not necessary to download and install any software. Use FormsPal's free PDF editor to complete, sign, and save the form directly in your browser. Follow these steps to get started:
Step 1: Click on the "Get Form" button in the top area of this webpage to open our PDF editor.
Step 2: This editor provides you with the ability to work with the PDF in various ways. Add your own text, adjust existing content, and add a signature, all in one place.
This PDF form will require particular information to be entered, so take the time to fill in what is asked:
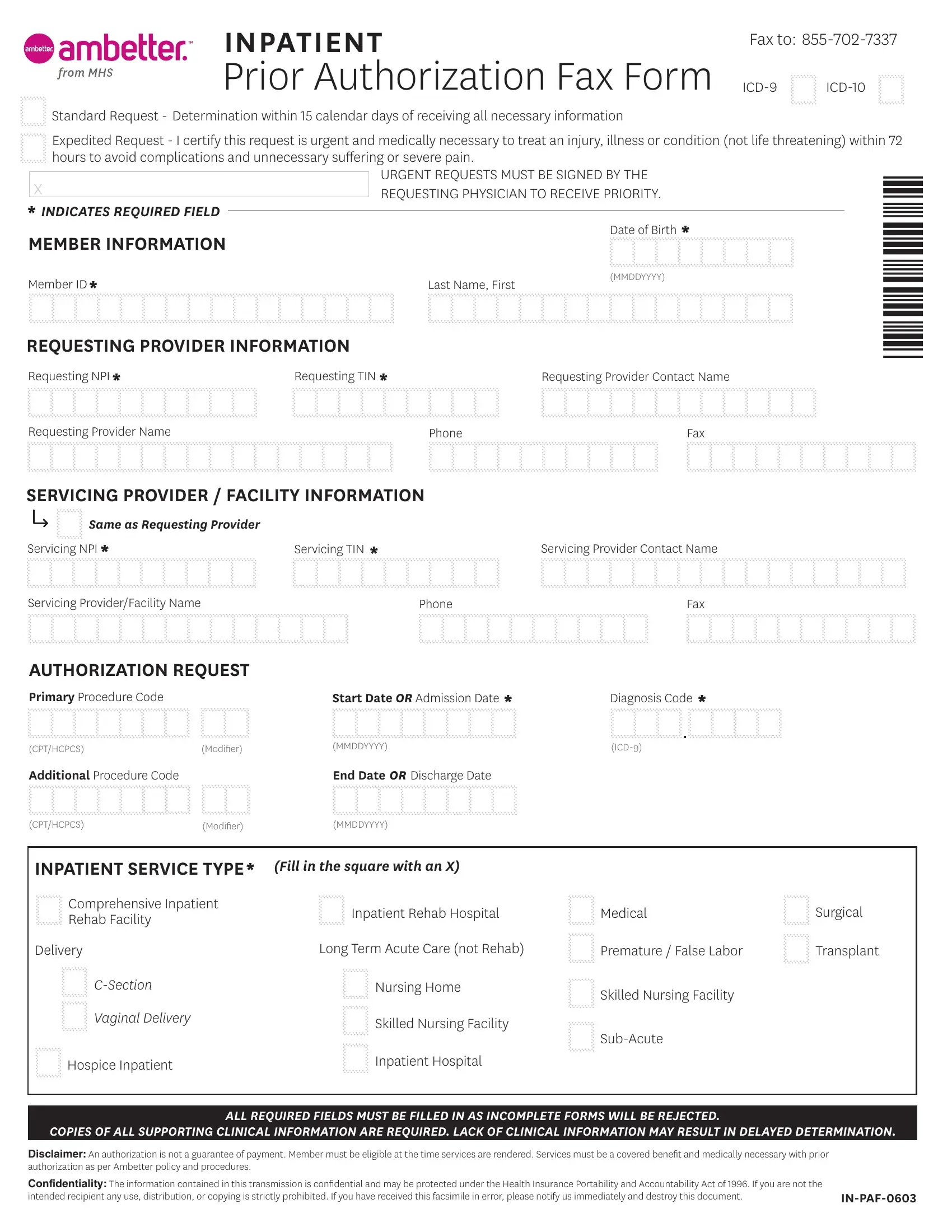
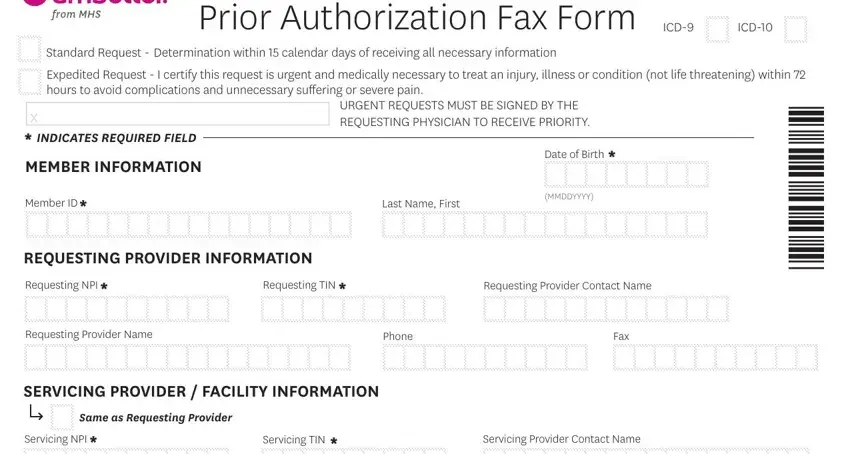
1. Fill out the member and provider details section. Collect all necessary information and make sure nothing is overlooked.
2. Enter the required specifics in the Servicing Provider/Facility Name, Phone, Fax, and the AUTHORIZATION REQUEST section, including Primary Procedure Code, Start Date or Admission Date, Diagnosis Code, CPT/HCPCS, Modifier, ICD, Additional Procedure Code, End Date or Discharge Date, CPT/HCPCS, and Modifier fields to complete the authorization request section.
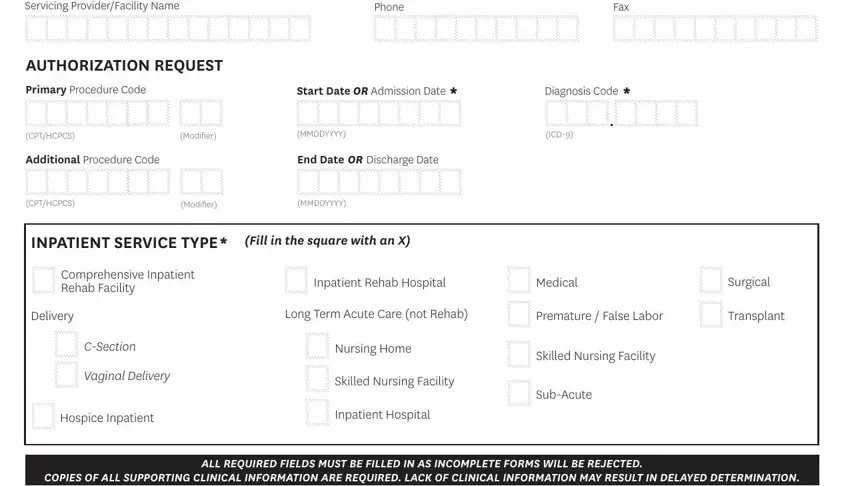
Be careful when filling out the CPT/HCPCS and Diagnosis Code fields, since these are where errors most often occur.
Step 3: Review all fields before finalizing. Once you are satisfied, click "Done." Sign up with FormsPal to access the Ambetter Inpatient Prior Authorization form, ready for download. All changes are saved so you can return and edit the document later if needed. We do not sell or share the details you provide when completing documents at FormsPal.
Frequently Asked Questions About the Ambetter Inpatient Prior Authorization Form
How long does prior authorization approval take for inpatient services?
Standard inpatient prior authorization requests receive a determination within 15 calendar days after Ambetter receives all required information and supporting clinical documentation. Expedited requests, reserved for urgent cases where a delay would cause serious harm to the patient, are processed within 72 hours.
What happens if I submit incomplete information on the Ambetter Inpatient Prior Authorization form?
Incomplete submissions or missing clinical data result in processing delays. Ambetter will not issue a determination until all required information is received. Always attach supporting physician notes, diagnostic reports, and any relevant lab results to avoid delays in the review process.
Does an approved prior authorization guarantee payment for inpatient services?
No. An authorization confirmation means Ambetter has reviewed the medical necessity of the requested inpatient service, but actual payment remains subject to the member's eligibility on the date of service and all applicable plan terms. Confirm the member's current benefit coverage before proceeding with inpatient care.
Providers filing related prior authorization requests may also need the Aetna Pharmacy Prior Authorization form for pharmacy benefit cases or the Healthnet Prior Authorization form for Healthnet plan members.