
How to Complete DD Form 1556-1
Follow these steps to fill out the training request and authorization form correctly for DoD personnel:
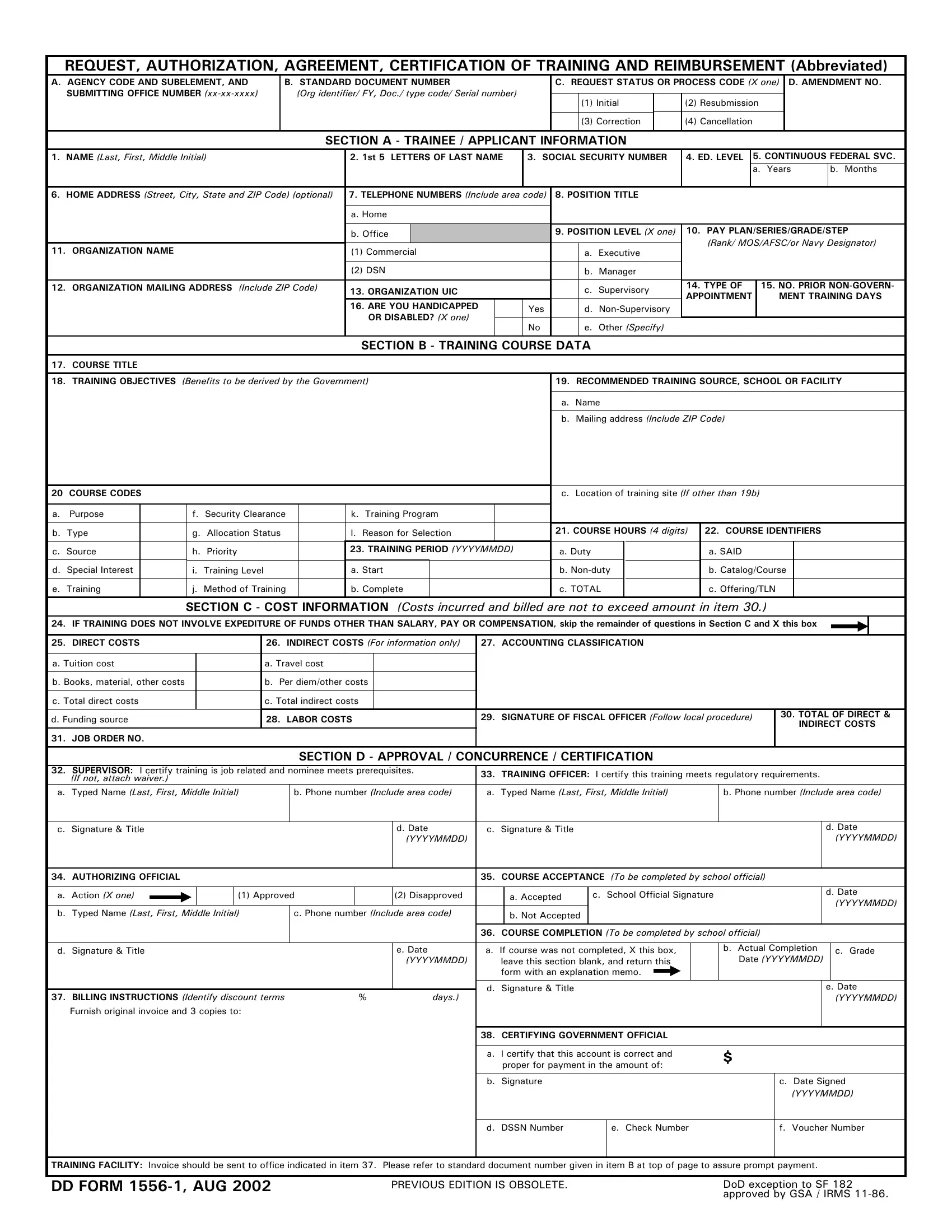
- Enter Trainee Information - Fill in your full name, Social Security Number, pay plan, grade, position title, and supervisor contact. All DoD civilian employees and military personnel must complete this section accurately.
- Provide Training Course Details - Enter the course title, course number, training provider name, training dates, and the location of the training facility. Include the course objective and the recommended number of training hours.
- List All Training Costs - Break down all expenses into direct costs (tuition, registration fees, required materials), indirect costs (travel and per diem), and labor costs (salary paid during training hours). All cost fields require supporting documentation from your training office.
- Obtain Supervisor Approval - Your supervisor must sign and date the form to confirm the training aligns with your position duties. Training officers and authorizing officials also review and sign the request before it advances.
- Review the Service Agreement - If training costs reach $1,000 or more, you must sign the service agreement section committing to continued federal employment for a set period following course completion.
- Submit Your Request - Submit the completed form to your human resources or training office. Keep a personal copy along with any written approval notices you receive from the authorizing official.
Who Files This Form
The form applies to civilian employees of the Department of Defense and to military personnel seeking employer-funded or reimbursed training programs. It is also required when a DoD employee attends courses funded through government contracts or interagency agreements. Related forms filed alongside this request include the OPM SF-182 Training Authorization, the Training Request Form, and the Military Training Request.
Frequently Asked Questions
What information does the form collect?
The form collects trainee identification and personal data, the specific training course details and objectives, a complete cost breakdown, supervisor endorsements, and a post-course evaluation and completion record. This makes it a full lifecycle document from initial request through reimbursement.
Is DD Form 1556-1 the same as SF-182?
No. The DD Form 1556-1 is specific to Department of Defense civilians and military personnel. The SF-182 is the government-wide training request form used across all federal agencies. Both serve similar purposes but follow different approval chains and include agency-specific requirements.
What happens if I leave my position after training?
When training costs reach $1,000 or more, the service agreement requires continued employment for a period proportional to the training investment. Early departure can result in prorated repayment obligations determined by your agency.
How long does the approval process take?
Approval timelines vary by agency and training cost. Requests typically move through supervisor, training officer, and authorizing official review within 5 to 15 business days. Urgent training needs may qualify for expedited review at the discretion of the authorizing official.
For related forms, see the DD Form 1351-2 Travel Voucher for travel reimbursement or the DD Form 1556 for the base training request document.