
How to Fill Out Alabama Form 390 Step by Step
Follow these steps to complete the form correctly and avoid delays in the approval process:
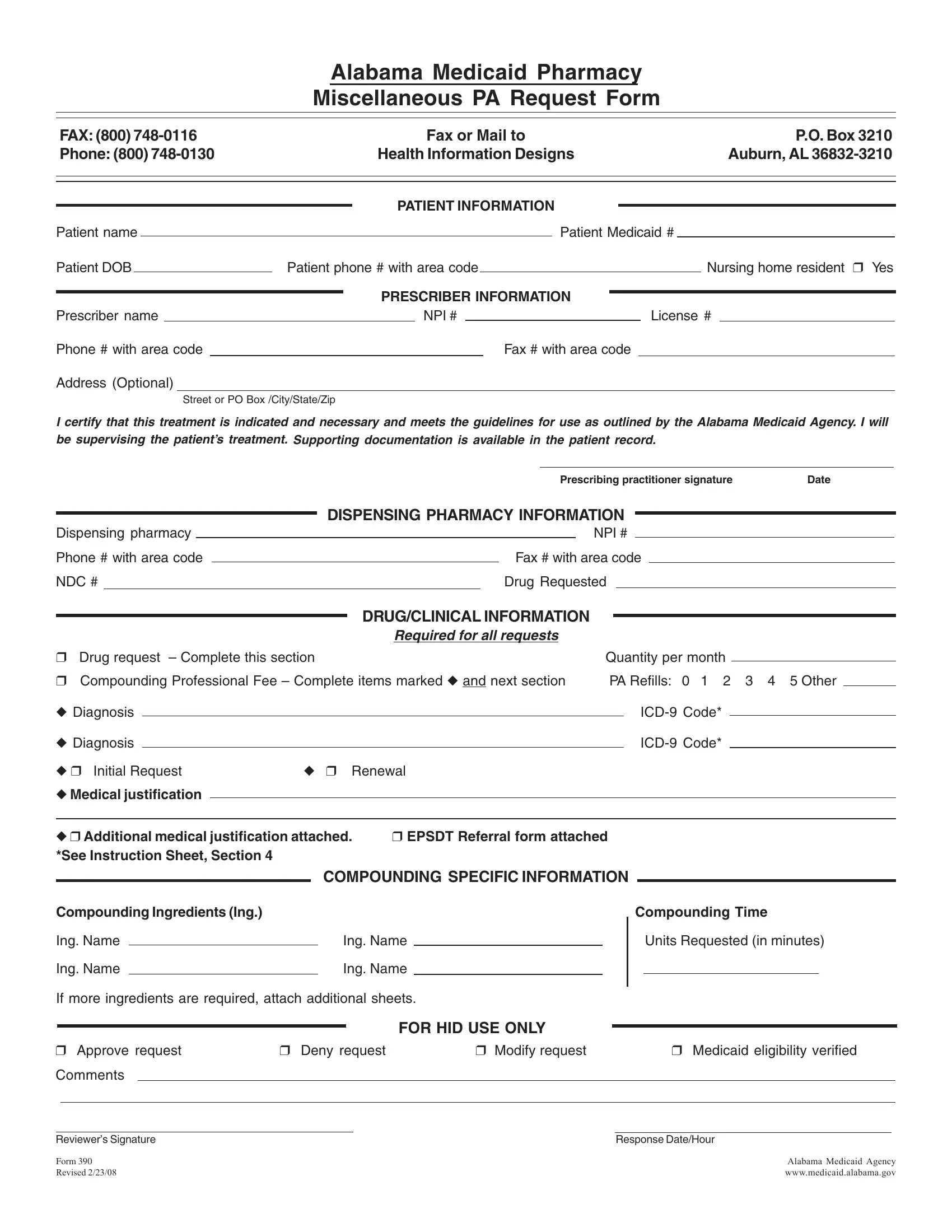
- Enter patient information. Write the patient's full name, Medicaid ID number, and date of birth in the fields at the top of the form.
- Add prescriber details. Include the prescriber's full name, NPI number, state license number, and contact phone number.
- Fill in pharmacy information. Enter the dispensing pharmacy name, phone number, fax number, and NPI.
- Specify the drug requested. Enter the drug name, NDC code, strength, and quantity. Include the number of days, weeks, or months of treatment being requested.
- Provide diagnosis codes. List the ICD-9 or ICD-10 diagnosis codes that support the medication request.
- Write the medical justification. Explain why the requested drug is medically necessary. Reference relevant clinical guidelines or prior treatment attempts with alternative medications where available.
- Complete the EPSDT section. If the request involves Early and Periodic Screening, Diagnostic, and Treatment services for a Medicaid recipient under age 21, check the appropriate box.
- Sign and date the form. The prescribing practitioner must sign and date the certification to confirm the accuracy of the information.
- Submit the completed form. Fax or mail the form to Health Information Designs at the address or fax number listed on the form.
Common Mistakes to Avoid
Healthcare providers frequently encounter delays due to these errors on Alabama Form 390:
- Leaving the NPI blank for either the prescriber or the dispensing pharmacy
- Using outdated ICD-9 codes where ICD-10 codes are now required
- Omitting the medical justification or writing a generic reason that does not reference the patient's specific clinical situation
- Failing to check the EPSDT box for eligible patients under age 21
- Submitting the form without the prescriber's signature and date
Frequently Asked Questions About Alabama Form 390
Who submits Alabama Form 390?
The form is submitted by the prescribing physician or the dispensing pharmacy on behalf of the patient. Either party can initiate the prior authorization request with Alabama Medicaid.
Where do you send Alabama Form 390?
Completed forms are sent to Health Information Designs (HID), which manages prior authorization requests for the Alabama Medicaid program. The fax number and mailing address are printed on the form.
How long does prior authorization take?
Alabama Medicaid typically processes non-urgent prior authorization requests within 3 business days. Urgent medical requests may be processed within 24 hours.
What happens if the request is denied?
If the prior authorization is denied, the prescriber receives a written notice explaining the reason. The prescriber can appeal by submitting additional clinical documentation to support the request. Patients may also request a fair hearing through the Alabama Medicaid Agency.
Can Form 390 be used for all medications?
No. Form 390 covers miscellaneous pharmacy requests only. Other medications may require a different prior authorization form. Check the Alabama Medicaid pharmacy guidelines to confirm which form applies to the specific drug. For mental health medications, providers may also need to complete an antipsychotic prior authorization form depending on the drug category.